
Brain
Expert Pharmacologist
- Joined
- Jul 6, 2021
- Messages
- 223
- Reaction score
- 197
- Points
- 43
Clinical effects and doses.
General effects of psilocybin are usually dose-dependent, and they include physiological, visual, auditory, cognitive, transpersonal and multisensory effects (e.g. synesthesia). There is a big difference in effects between a low and a high dose of psilocybin. For example, high doses induce extreme agitation with significant visual distortion, while low doses cause mild sedative effect and increase visual acuity. "Body high" effect is described as a light pleasant tingling sensation that involves the whole body and creates a sensation of “glowing weightlessness”. The range of effects is summarized in the table below. Psilocybin mildly stimulates sympathetic activity (mydriasis, moderate increase in blood pressure and increase in heart rate) at a dose 3-5 mg and full effect at a dose 10-25 mg. The increase in systolic and diastolic blood pressure is approximately 10-30 mmHg. Average heart rate ranges from 80-90 bpm with the maximum of 140 bpm. Psilocybin doesn’t affect ECG and body temperature. Other common somatic symptoms of psilocybin use include: dizziness, weakness, tremor, nausea and vomiting (after consuming psilocybin-containing mushrooms), drowsiness, yawning, paresthesia, blurred vision and increased tendon reflexes. Psilocybin does not acutely affect the ionic balance, blood glucose or cholesterol, and even in high doses has only a negligible effect on plasma concentration or the activity of various enzymes (lactate dehydrogenase, alanine transaminase, alkaline phosphatase and cholinesterase, mild elevation of aspartate aminotransferase and γ-glutamyl transferase). However, psilocybin increases levels of prolactin, and in high doses also corticotropin, cortisol and thyreotropin. Hormone levels have returned to normal within five hours. Low doses of psilocybin cause drowsiness and intensify the mood, which is present at the moment of use, stabilize and enhance it. Medium doses of the substance induce stable, controllable consciousness alteration; higher doses induce intense psychedelic experience. Phenomenology of psilocybin intoxication includes alteration of perception, characterized by states of pseudodreams, illusions, hallucinations, synesthesia, changes in body image (for example, tingling paresthesia, daydreaming or somatic hallucinations), altered self-perception, derealization and depersonalization, impaired perception of time and space, attention disorder, thought content disorder (magical thinking, unusual ideas or delirium), a change in intuition, and sometimes a sharp mood swing, symptoms of anxiety or euphoria, impaired concentration and nervousness. Emotions during psilocybin trip can vary from ecstatic and pleasant to anxiety. In scientific world, psilocybin effects (as well as other hallucinogens) are evaluated using a rating scale ASCs and 5 subscales of altered state of consciousness, АED and VUS. Psilocybin affects some areas responsible for cognitive function and information processing. It also decreases the ability to visually distinguish faces with negative or neutral expression, but not positive-neutral expressions. It disrupts sustained attention, changes the processing of visual information.
Psilocybin affects sensorimotor gating (PPI), which is impaired at short intervals. It is known that psilocybin induces numerous mystic spiritual experiences, which was first registered in a famous experiment of Pankhe in 1963. These groundbreaking experiments have been recently confirmed by a double-blind controlled trial, which concluded that, psilocybin trip experience is described as one having personal meaning and spiritual significance with sustained positive changes in attitude and behavior. According to the results of numerous studies, psilocybin doesn't have specific gastrointestinal or cardio toxicity. Theoretical median lethal dose in humans is assumed to be 20 g of pure substance. The safety of psilocybin use is given mainly by personal expectations (set) and the nature of the environment (setting), which is the cause of the great variability of the subjective effects. Due to the altered perception, hallucinations and intensified emotions, dangerous behavior may occur during nonmedical administration. These complications can be significantly reduced by educating an individual, creating a safe environment and building rapport with an experienced intoxication guide (sitter). Thus, well-prepared hallucinogen-naïve participants can safely take higher doses of psilocybin (over 25 mg). The most common side effects of psilocybin are: tachycardia, anxiety, nausea, vomiting, diarrhea, emotional lability, hallucinations, a sense of impending death and confusion. Nausea is one of the most common side effects, associated with consuming the flesh of the mushroom, not psilocybin itself. More serious side effects include HPPD-syndrome. Risk of convulsions is low; however, it is still considered a side effect. Probability of developing convulsions increases when exposed to exogenous or endogenous stress, fatigue or dehydration during use. Simultaneous tramadol intake, which is μ-opioid receptor agonist with additional properties of serotonin and noradenaline reuptake, can increase the risk of convulsions due to its potential to lower the seizure threshold. Damage to heart valves is possible when psilocybin is used frequently for long-term due to 5-НТ2В receptor activity, which induces proliferation of cardiac, leading to an increase in the "rigidity" of the valves. Risk of interactions between psilocybin and other drugs, food products and diseases is constant. For example, one of the most dangerous interactions is the interaction with tramadol, which lowers seizure threshold. Synergic reactions, enhancing psychedelic action of psilocybin, can be expected in combination with other psychedelics, inhibiting psilocybin's metabolism (e.g. MAO inhibitors). Drugs that do not show synergy, but can alter the course of psilocybin trip by enhancing agitation or causing drowsiness instead, include psychostimulants and opioid receptors agonists. Certain drugs able to weaken psilocybin action are: ethanol, gamma-hydroxybutyric acid (GHB), SSRI, benzodiazepines. When using cannabis together with psilocybin, pronounced relaxation and/or intense anxiety can occur. When using amphetamines together with psilocybin, the risk of a “thought loop”, when user can't get rid of a repeated pattern of thoughts and ideas, increases. Generally, although the use of hallucinogens can trigger nonspecific psychotic episodes or accentuate psychotic symptoms in patients, these substances are not the etiological agents. The risk of prolonged psychosis (lasting longer than 48 hours) in otherwise healthy subjects after a single dose of psilocybin is rare, and in most cases it is associated with personality predisposition. The prevalence of prolonged psychiatric symptoms after serotonergic hallucinogens in thousands of healthy subjects and psychiatric patients was 0.08- 0.09 % and 0.18 %, respectively. Attempts to commit suicide occurred in psychiatric patients only (in 0.12 %) with few (0.04 %) succeeding. Finally, incidence of HPPD is estimated to be in only a few cases per million users. Since chronic administration of hallucinogens reduces the number of 5HT2A receptors leading to a rapid onset of short-lasting tolerance, the risk of addiction to hallucinogens, including psilocybin is very low. Furthermore, monkeys did not seek psilocybin as a reward, and in the case of LSD, they even reacted aversely. In humans, psilocybin does not cause craving or withdrawal, and it does not directly affect the mesolimbic dopaminergic pathway and therefore does not activate the reward system. Electrophysiological studies, limited by visual evaluation, determine an increase in rapid activity and a decrease in amplitude and desynchronization in people using psilocybin. A decrease in alpha and theta activity is also registered. The recent studies on psilocybin have demonstrated a decrease in the absolute power and coherence of the EEG (mainly front-temporal), the relative power decreases in the delta and theta ranges and increases in the alpha, beta, and gamma ranges.
General effects of psilocybin are usually dose-dependent, and they include physiological, visual, auditory, cognitive, transpersonal and multisensory effects (e.g. synesthesia). There is a big difference in effects between a low and a high dose of psilocybin. For example, high doses induce extreme agitation with significant visual distortion, while low doses cause mild sedative effect and increase visual acuity. "Body high" effect is described as a light pleasant tingling sensation that involves the whole body and creates a sensation of “glowing weightlessness”. The range of effects is summarized in the table below. Psilocybin mildly stimulates sympathetic activity (mydriasis, moderate increase in blood pressure and increase in heart rate) at a dose 3-5 mg and full effect at a dose 10-25 mg. The increase in systolic and diastolic blood pressure is approximately 10-30 mmHg. Average heart rate ranges from 80-90 bpm with the maximum of 140 bpm. Psilocybin doesn’t affect ECG and body temperature. Other common somatic symptoms of psilocybin use include: dizziness, weakness, tremor, nausea and vomiting (after consuming psilocybin-containing mushrooms), drowsiness, yawning, paresthesia, blurred vision and increased tendon reflexes. Psilocybin does not acutely affect the ionic balance, blood glucose or cholesterol, and even in high doses has only a negligible effect on plasma concentration or the activity of various enzymes (lactate dehydrogenase, alanine transaminase, alkaline phosphatase and cholinesterase, mild elevation of aspartate aminotransferase and γ-glutamyl transferase). However, psilocybin increases levels of prolactin, and in high doses also corticotropin, cortisol and thyreotropin. Hormone levels have returned to normal within five hours. Low doses of psilocybin cause drowsiness and intensify the mood, which is present at the moment of use, stabilize and enhance it. Medium doses of the substance induce stable, controllable consciousness alteration; higher doses induce intense psychedelic experience. Phenomenology of psilocybin intoxication includes alteration of perception, characterized by states of pseudodreams, illusions, hallucinations, synesthesia, changes in body image (for example, tingling paresthesia, daydreaming or somatic hallucinations), altered self-perception, derealization and depersonalization, impaired perception of time and space, attention disorder, thought content disorder (magical thinking, unusual ideas or delirium), a change in intuition, and sometimes a sharp mood swing, symptoms of anxiety or euphoria, impaired concentration and nervousness. Emotions during psilocybin trip can vary from ecstatic and pleasant to anxiety. In scientific world, psilocybin effects (as well as other hallucinogens) are evaluated using a rating scale ASCs and 5 subscales of altered state of consciousness, АED and VUS. Psilocybin affects some areas responsible for cognitive function and information processing. It also decreases the ability to visually distinguish faces with negative or neutral expression, but not positive-neutral expressions. It disrupts sustained attention, changes the processing of visual information.
Psilocybin affects sensorimotor gating (PPI), which is impaired at short intervals. It is known that psilocybin induces numerous mystic spiritual experiences, which was first registered in a famous experiment of Pankhe in 1963. These groundbreaking experiments have been recently confirmed by a double-blind controlled trial, which concluded that, psilocybin trip experience is described as one having personal meaning and spiritual significance with sustained positive changes in attitude and behavior. According to the results of numerous studies, psilocybin doesn't have specific gastrointestinal or cardio toxicity. Theoretical median lethal dose in humans is assumed to be 20 g of pure substance. The safety of psilocybin use is given mainly by personal expectations (set) and the nature of the environment (setting), which is the cause of the great variability of the subjective effects. Due to the altered perception, hallucinations and intensified emotions, dangerous behavior may occur during nonmedical administration. These complications can be significantly reduced by educating an individual, creating a safe environment and building rapport with an experienced intoxication guide (sitter). Thus, well-prepared hallucinogen-naïve participants can safely take higher doses of psilocybin (over 25 mg). The most common side effects of psilocybin are: tachycardia, anxiety, nausea, vomiting, diarrhea, emotional lability, hallucinations, a sense of impending death and confusion. Nausea is one of the most common side effects, associated with consuming the flesh of the mushroom, not psilocybin itself. More serious side effects include HPPD-syndrome. Risk of convulsions is low; however, it is still considered a side effect. Probability of developing convulsions increases when exposed to exogenous or endogenous stress, fatigue or dehydration during use. Simultaneous tramadol intake, which is μ-opioid receptor agonist with additional properties of serotonin and noradenaline reuptake, can increase the risk of convulsions due to its potential to lower the seizure threshold. Damage to heart valves is possible when psilocybin is used frequently for long-term due to 5-НТ2В receptor activity, which induces proliferation of cardiac, leading to an increase in the "rigidity" of the valves. Risk of interactions between psilocybin and other drugs, food products and diseases is constant. For example, one of the most dangerous interactions is the interaction with tramadol, which lowers seizure threshold. Synergic reactions, enhancing psychedelic action of psilocybin, can be expected in combination with other psychedelics, inhibiting psilocybin's metabolism (e.g. MAO inhibitors). Drugs that do not show synergy, but can alter the course of psilocybin trip by enhancing agitation or causing drowsiness instead, include psychostimulants and opioid receptors agonists. Certain drugs able to weaken psilocybin action are: ethanol, gamma-hydroxybutyric acid (GHB), SSRI, benzodiazepines. When using cannabis together with psilocybin, pronounced relaxation and/or intense anxiety can occur. When using amphetamines together with psilocybin, the risk of a “thought loop”, when user can't get rid of a repeated pattern of thoughts and ideas, increases. Generally, although the use of hallucinogens can trigger nonspecific psychotic episodes or accentuate psychotic symptoms in patients, these substances are not the etiological agents. The risk of prolonged psychosis (lasting longer than 48 hours) in otherwise healthy subjects after a single dose of psilocybin is rare, and in most cases it is associated with personality predisposition. The prevalence of prolonged psychiatric symptoms after serotonergic hallucinogens in thousands of healthy subjects and psychiatric patients was 0.08- 0.09 % and 0.18 %, respectively. Attempts to commit suicide occurred in psychiatric patients only (in 0.12 %) with few (0.04 %) succeeding. Finally, incidence of HPPD is estimated to be in only a few cases per million users. Since chronic administration of hallucinogens reduces the number of 5HT2A receptors leading to a rapid onset of short-lasting tolerance, the risk of addiction to hallucinogens, including psilocybin is very low. Furthermore, monkeys did not seek psilocybin as a reward, and in the case of LSD, they even reacted aversely. In humans, psilocybin does not cause craving or withdrawal, and it does not directly affect the mesolimbic dopaminergic pathway and therefore does not activate the reward system. Electrophysiological studies, limited by visual evaluation, determine an increase in rapid activity and a decrease in amplitude and desynchronization in people using psilocybin. A decrease in alpha and theta activity is also registered. The recent studies on psilocybin have demonstrated a decrease in the absolute power and coherence of the EEG (mainly front-temporal), the relative power decreases in the delta and theta ranges and increases in the alpha, beta, and gamma ranges.
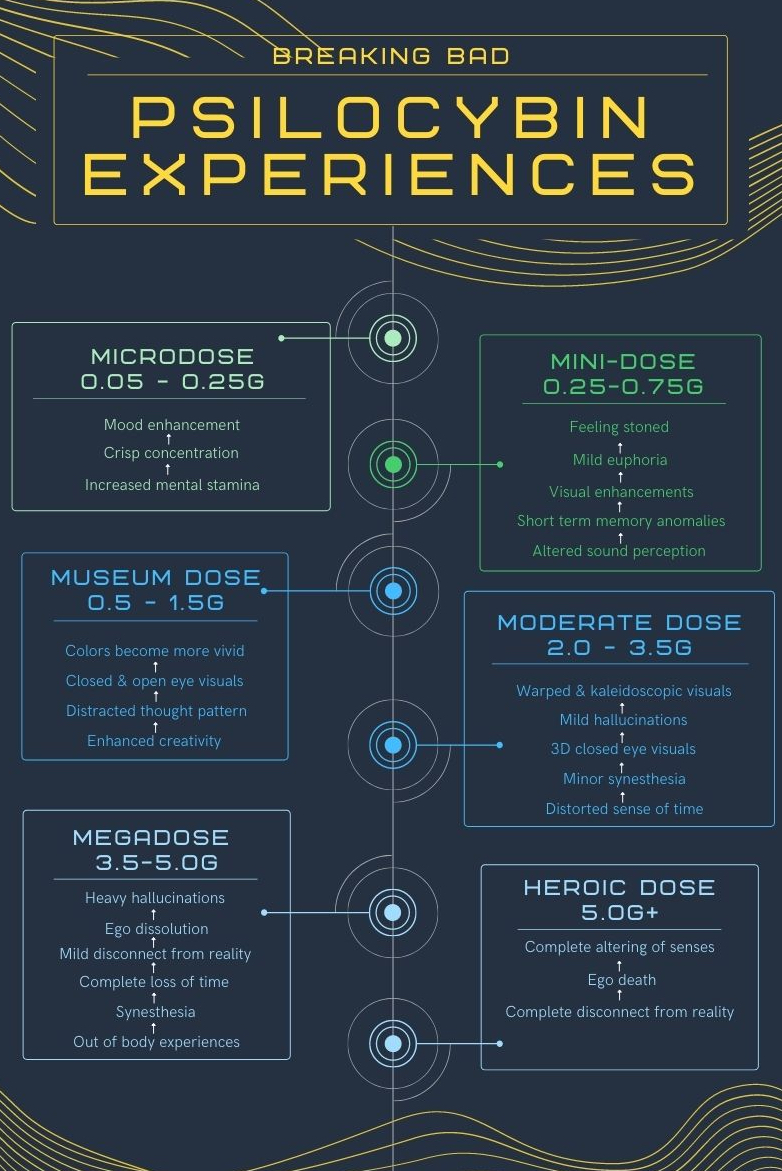
Microdose (0.05-0.25 g).
A microdose is a sub-perceptual (unnoticeable) dose, which many people incorporate into their weekly routines. The idea behind this is to enhance levels of creativity, energy, and focus, and decrease levels of stress, anxiety, and emotional instability. Find out more in our microdosing guide. Common effects include:mood enhancement, decreased stress, emotional stability, mindfulness, presence, peace; openness and self-forgiveness; conversational fluidity; alleviation of persistent conditions such as depression, anxiety, ADD/ADHD, and PTSD; increased motivation (e.g. to make positive lifestyle changes); increased flow states; clearer, more connected thinking; improved memory; increased creativity; easier meditation; enhanced athletic endurance; increased energy overall (without anxiety or a subsequent crash); slight amplification of mood, positive or negative; possible manic states; potentially increased neuroticism.
Mini-dose (0.25-0.75 g).
While a proper microdose shouldn’t be felt, a mini-dose of psilocybin takes you just above the perceptual threshold—but it’s not a full-blown trip. As one of our community members put it, a mini-dose gives you “that total expansion of being, total free flow feeling” without losing touch with your surroundings. Common effects include: mood enhancement; mild euphoria or excitement; mindfulness, presence, and peace; openness and self-forgiveness Introspective insights; alleviation of persistent conditions such as depression, anxiety, ADD/ADHD, and PTSD; increased motivation (e.g. to make positive lifestyle changes) Increased flow states; clearer, more connected thinking; enhanced senses; easier meditation; increased enjoyment of physical activity and everyday tasks; preference for introspection over socializing Increased sensitivity to light; very mild visuals, if any; possible manic states; difficulty focusing or thought loops; difficulty with some cognitive tasks; anxiety, agitation, or restlessness; difficulty or discomfort socializing.
Museum dose (0.5-1.5 g).
The effects of psilocybin are more apparent with a museum dose than with a mini-dose, but a museum dose still won’t give you a full psychedelic experience. The name “museum dose,” coined by the biochemist and pharmacologist Dr. Alexander Shulgin, refers to the fact that on this dose, you can still participate in public activities (such as viewing paintings in a museum) without attracting attention. Common effects include: mood enhancement, euphoria or excitement; mild to moderate visuals (e.g. “breathing” environments); increased empathy; conversational fluidity; introspection Increased flow states; enhanced senses enhanced appreciation for music, art, etc.; increased creativity; amplification of mood, positive or negative; altered perception of sound; time dilation or contraction (time passing more slowly or quickly); increased sensitivity to light; pupil dilation; difficulty focusing or thought loops; difficulty or discomfort socializing; frustration at dosage (the “no man’s land”).
Moderate dose (2-3.5 g).
This is where the full psychedelic experience begins. You’ll likely see visual hallucinations, including patterns and fractals, and things like time and depth perception will be distorted. But with this dose, you’re still able to grasp your surroundings—they’ll just be highly altered. Common effects include: life-changing introspective or philosophical insights; increased flow of ideas; enhanced appreciation for music, art, etc.; finding otherwise mundane things funny or interesting; clear come-up, peak, and come-down; amplification of emotions, whether good or bad; open- and closed-eye visuals (e.g. patterns, auras); synesthesia; sensitivity to light; compulsive yawning; disorientation; fear and anxiety (“bad trip” experiences); difficulty with cognitive tasks; dizziness; nausea.
Megadose (5+ g).
A megadose brings on a total loss of connection with reality. This is where you’ll experience intense hallucinations, as well as ego death, mystical experiences, and deep introspection. Common effects include: mystical experience and intense feelings of wonder; life-changing introspective or philosophical insights; ego death; very strong open- and closed-eye visions (e.g. memories coming to life); synesthesia; time becoming meaningless; disorientation; compromised motor functions (sitter recommended!); strong fear and anxiety (extreme “bad trip” experiences); extreme difficulty with cognitive tasks; dizziness; nausea.
In a survey of roughly 2000 participants who reported having challenging experiences after ingesting psilocybin mushrooms, 39% reported the experiences as one of the top 5 most challenging experiences of their lifetime. Additionally, 11% reported putting themselves or others at risk of physical harm, 2.6% reported having aggressive or violent behavior, and 2.7% reported getting medical help during the “bad trip”. The rates and severity of problems from the survey were notably higher than those observed in laboratory research settings that are carefully screened, prepared, and monitored. Overall, the survey showed difficult experiences associated with psilocybin as acute psychological distress, dangerous behavior, and enduring psychological problems. Extrinsic factors of a non-laboratory controlled environment can make the experience more difficult and more harmful for those involved. Despite these difficulties, 84% reported having benefited from the experience. The degree of difficulty of the challenging experience as well as personal and spiritual significance and increased life satisfaction were positively correlated. Another large survey demonstrated that increased neuroticism is associated with greater intensity of the challenging experience with psilocybin. It is shown that those with high negative schizotypy typically experience negative and stressful reactions to altered states of consciousness, such as is induced by psilocybin. Even in optimal settings and conditions such as clinical trials, subjects can still face challenging trips. The influence of external environmental confounding factors can make these bad experiences more likely as well as prolonged. In a study on the immediate and persisting effects of psilocybin, 39% reported that they had an extreme experience of fear, fear of insanity, or feeling trapped during the session, usually during the highest dosage. There was a positive correlation between dosage and ratings of fear or anxiety, but there was varying on set and duration for each subject. Forty-four percent had delusions or paranoia, again most subjects experiencing this after the highest dose. Generally, there were positive ratings of attitudes on life, attitudes on self, mood, social effects, and behavior following the experience. Despite these challenges, none of the subjects reported feeling a decreased sense of well-being or life satisfaction. None reported bothersome or clinically significant persisting perception phenomena, and there were no reports of future non- study related uses of hallucinogens since. Of those that reached the full criteria for completing a mystical experience, spiritual significance also did not change over time. In fact, 61% rated the two highest doses to be the single most spiritually significant experiences of their lives, 83% rating it in their top five. Eighty-nine percent indicated those sessions increased well-being or life satisfaction and positively changed their behavior at least moderately.
Psilocybin is 45 times less effective than LSD and 66 times more effective than mescaline. Clinical trials have proven the effective dose for oral administration of psilocybin to be 0.045-0.429 mg/kg for adult human (for intravenous administration the dose is about 1-2 mg of psilocybin). Psychodelic effects manifest at a dose more than 15 mg orally, or at psilocin level in blood plasma of 4-6 ng/ml. In safety recommendations on experimental hallucinogen use, it is stated that high, but non-dangerous dose of psilocybin for oral administration is any dose which doesn't exceed 25 mg. The onset of action is within 20-40 minutes, maximum - 60-90 minutes. The duration is about 4-6 hours after oral administration. The main effects are leveled within 8 hours; all the effects are leveled completely within 24-30 hours. When used intravenously, effects of psilocybin begin within 1-2 minutes, reach their peak within 4-5minutes and last for about 1 hour. As for microdosing, there are very few studies on this method of use. The history of microdosing is very unclear, but it is known that Albert Hoffman, the chemist who discovered LSD, started microdosing in later periods of his life in the 1990s. Before the ban on psychedelic research in 1966, no studies on microdosing had been carried out. Some progress has been made in starting the process of studying microdosing officially. Some researchers are trying to prove their point, while others carry out primary clinical trials to determine safety of the microdosing research. People try microdosing to relieve mental illness symptoms such as anxiety and depression, while others try to boost their productivity and creative potential in solving problems. Microdose is considered a subperceptual dose, it doesn't cause any acute effects. When the user is administrated a microdose, they will not feel any effects or feel high. Most users microdose psilocybin to relieve symptoms of depression and anxiety and to improve both convergent and divergent thinking. The study as of 2018 showed preliminary results, which confirmed the statement about convergent and divergent thinking. A typical microdose makes up the tenth part of the normal dose. Doctor Fadiman, an active supporter of microdosing and psychedelic research, recommends taking 0,2 g of dried mushrooms every 3 or 4 days. Ensuring constant dosing is considered to be one of the most important aspects. Dosing refers to dosage of substance and also to frequency and duration of use. Microdose is so little that it is easy to accidentally take a higher dose than expected. Psilocybin-containing mushrooms make it even more difficult because of different strength of different types of individual mushrooms. One example of this is the differences in efficacy between cup and stem of psilocybin-containing mushrooms. The study, dedicated to analysis of psilocybin-containing mushrooms in Japan, showed that maximum efficacy of P. cubensis is 1.27% in stem and 1.35% in cap. This study also showed that whole mushrooms have the efficacy from 0.37% to 1.30%.
Prospects of psilocybin development.
Psilocybin has been a subject of preliminary research since the early 1960s, when the Harvard Psilocybin Project evaluated the potential therapeutic value of psilocybin for personality disorders. Beginning in the 2000s decade, research on anxiety disorders, major depression, and various addictions was conducted. Psilocybin has been tested for its potential for developing prescription drugs to treat drug dependence, anxiety, or mood disorders. There is evidence that psilocybin and LSD induce molecular and cellular adaptations related to neuroplasticity, and that these could potentially underlie therapeutic benefits. In 2018-19, the United States Food and Drug Administration (FDA) granted Breakthrough Therapy Designation for psilocybin-assisted therapy for treatment-resistant depression and major depressive disorder, a review process enabling the FDA to implement an expedited review if clinical research results for psilocybin use in treating depression are compelling. A 2021 review found use of psilocybin was associated with reduced intensity of depression symptoms. As of 2021, many new centers for psychedelic research exploring the use of psilocybin have been launched, including the Centre for Psychedelic Research at Imperial College London, the UC Berkeley Center for the Science of Psychedelics, the Center for Psychedelic and Consciousness Research at Johns Hopkins University, and the Psychae Institute in Melbourne.
For instance, in recent studies unambiguously positive effects of psilocybin have been identified in treatment of depression, which have sufficient duration, ideal safety and tolerability, compared to any other known antidepressants. The mechanism of antidepressive effect, according to the study, is assumed to be associated with stimulation of neuron plasticity and change in functioning of the neural network, presumably due to 5НТ2А agonism of psilocybin. Also, there are internal factors, such as person's "expectation" and external factors (setting, which psilocybin is used in). The importance of “set” and “setting” in psychedelic-assisted therapy was emphasized by Timothy Leary in the 1960s. Whereas “set” refers to more internal factors, such as the personality, expectations, and state of mind of an individual when entering a psychedelic session, “setting” describes external factors, such as the physical and social environment of the session. A thorough review of the topic of set and setting, in addition to its history, can be found at Hartogsohn 2016 and 2017. Of note, “set”, “setting” and the type of psychedelic experience apparently may not only have an impact on the acute experience, but also on the long-term outcome of psilocybin-assisted therapy. In a trial involving 20 patients with treatment-resistant depression who received two doses of psilocybin in two separate sessions, the quality of the acute experience during the session appeared to be of major importance for long-term changes.
In a recent pilot, study psilocybin at low doses (0.2 mg/kg) acted as an anxiolytic and antidepressant in terminally ill cancer patients without clinically significant side effects. This study follows on from another three where effects on psychosocial distress/inner psychological well-being, anxiety and depression, attitudes to the disease and towards death, quality of life and spiritual/mystical states of consciousness, secondarily changes in the perception of pain and plasma markers of stress and immune system function are evaluated. Case reports and clinical trials have also reported improvement of obsessive- compulsive disorder (OCD) symptoms after psilocybin. In one patient, the effect persisted for five months. In studies devoted to the treatment of alcohol dependence and smoking cessation it is suggested that psilocybin deepens spirituality and stimulates motivation to overcome the addiction. Further on, a potential future use of psilocybin in the treatment of anxiety depressive disorder is also emerging. A high “mystical-type experience” was predictive, whereas anxiety and impaired cognition correlated negatively with a positive long-term outcome. A study evaluated potential predictive variables for the response to psilocybin in 261 healthy volunteers who underwent a total of 409 psilocybin administrations. They found that a high score in the personality trait of absorption, being in an emotionally excitable and active state immediately before drug intake, and the experience of few psychological problems in preceding weeks, were strongly associated with higher “mystical-type experiences” and pleasant experiences. In contrast, young age, emotional excitability, and an experimental setting (e.g., neuroimaging) predicted unpleasant or anxious reactions to psilocybin experiences. A prospective study using a web-based data collection to predict responses to psychedelics, not limited to psilocybin, also found a positive effect on well-being that was associated with a “mystical-type experience”. In addition, having clear intentions and the feeling of being ready for the experience had a positive impact on “mystical-type experience”, supporting the importance of “set” and “setting”. Several studies are ongoing to overcome some of the limitations mentioned and to shed light on some of the outstanding issues. One double-blind phase 2 trial conducted by the Usona Institute on psilocybin in the treatment of major depressive disorder is investigating 80 participants under the two conditions of a verum group receiving psilocybin 25 mg and an active placebo control with 100 mg niacin. The COMPASS Pathways study aims to gain information on the optimal dose of psilocybin in treatment-resistant depression. This study will compare the effects of 25 mg vs. 10 mg vs. 1 mg of psilocybin, and also aims to shed further light on the role and efficacy of microdosing. Another multicenter phase II trial called EPIsoDE will include 144 patients with treatment-resistant depression in a cross-over design.
In summary, psilocybin has a strong research and therapeutic potential. Due to the good knowledge of its pharmacodynamics and pharmacokinetics, beneficial safety profile and zero potential to cause addiction, it is frequently used both in animal and human research. It brings a number of key findings regarding the functioning of the human brain, in particular the role of the serotonergic system in complex functions such as perception and emotions. It also serves as a useful tool for the study of the neurobiology of psychoses. Due to its considerable degree of translational validity of animal and human studies, a psilocybin model of psychosis plays a key role in the development of new treatments for psychotic disorders. Finally, the most recent human studies also suggest its potential therapeutic use in the treatment of several psychiatric and neurological disorders.
- A New Understanding: The Science of Psilocybin—A 2019 documentary exploring psilocybin research for end-of-life anxiety in terminally ill cancer patients.
- Fantastic Fungi—A film by Louie Schwartzberg exploring the biology, environmental roles, and medicinal uses of fungi, including magic mushrooms.
- The Rise of Psychedelic Truffles in Amsterdam—A short documentary by Vice on the history of the legal loophole that allows psilocybin truffles to be sold legally in Amsterdam.
- Psilocybin Mushrooms & The Mycology of Consciousness—A talk by the mycologist Paul Stamets at Psychedelic Science 2017, a six-day gathering co-hosted by MAPS and the Beckley Foundation.
- The Science of Psilocybin and its Use to Relieve Suffering—A 2016 TED talk by Roland Griffiths on psilocybin’s ability to catalyze spiritual transformation and reduce existential fears in cancer patients.
- Magic Mushrooms in Mexico—Season 1, Episode 4 of Hamilton’s Pharmacopeia. The episode features Hamilton Morris, who examines the history and effects of psilocybin mushrooms with the help of scientists and shamans in Oaxaca.
- Magic Mushroom Medical Trial—A documentary from Real Stories that follows three volunteers and their families who are involved in a psilocybin clinical trial for depression.
- The Stoned Ape Theory—Terence McKenna explaining his Stoned Ape Theory.
- https://link.springer.com/article/10.1007/s00213-006-0457-5
- https://clinicaltrials.gov/ct2/show/NCT04052568
- https://journals.sagepub.com/doi/abs/10.1177/0269881111420188
- https://mapscontent.s3-us-west-1.am...locybin/JHU-Psilocybin-Cancer-Ed-JOP-2016.pdf
- https://www.nature.com/articles/s41598-020-59282-y
- https://clinicaltrials.gov/ct2/show/NCT02243813
- https://clinicaltrials.gov/ct2/show/NCT01943994
- https://clinicaltrials.gov/ct2/show/NCT04123314
- https://clinicaltrials.gov/ct2/show/NCT03554174
- https://clinicaltrials.gov/ct2/show/NCT03356483
- https://clinicaltrials.gov/ct2/show/NCT02981173
- https://journals.sagepub.com/doi/pdf/10.1177/0269881116675512
- https://clinicaltrials.gov/ct2/show/NCT02421263
- https://www.nyucanceranxiety.org/
The Department of Psychiatry, Psychotherapy, and Psychosomatics at the University of Zurich is a hub for psilocybin research in Europe. The university is home to the Heffter Research Center, which has conducted over 70 studies on the neuroscience of psychedelics with support from the Heffter Research Institute.
- https://clinicaltrials.gov/ct2/show/NCT03715127
- https://clinicaltrials.gov/ct2/show/NCT04141501
- https://www.sciencedirect.com/science/article/abs/pii/S0006322314002753
- https://maps.org/other-psychedelic-...effects_on_attention_perception_and_cognition
- https://clinicaltrials.gov/ct2/show/NCT03429075
- https://www.pnas.org/content/109/6/2138.short
- https://www.nature.com/articles/s41598-017-13282-7
- https://compasspathways.com/our-res...s/treatment-resistant-depression/#from-subnav
- https://compasspathways.com/our-res...apy/clinical-trials/healthy-volunteers-study/
- https://clinicaltrials.gov/ct2/show/NCT04433845
Last edited by a moderator: